

Can Damaged Milk Ducts Repair Themselves
Making breast size smaller in a surgical procedure is known every bit breast reduction. This article discusses how breast reduction surgery can affect milk supply, whether women who have had breast reduction surgery can still breastfeed and answers frequently asked questions. For data nigh breast augmentation run across Breastfeeding With Implants.
Breastfeeding afterwards chest surgery
To brand breast milk, a breast needs glandular or milk-making tissue and a neurohormonal reflex to release the milk (see box). Any kind of surgery on the breast has the potential to disturb milk production or milk release to some degree. How breastfeeding might be afflicted later breast reduction surgery volition depend on:
- The type of surgery involved—whether important nerves and milk ducts (tubes that carry milk to the nipple) have been cutting, whether the nipple has been repositioned, and whether the claret supply to the chest is intact.
- How much milk-making (glandular) chest tissue remains
- The length of time since the surgery
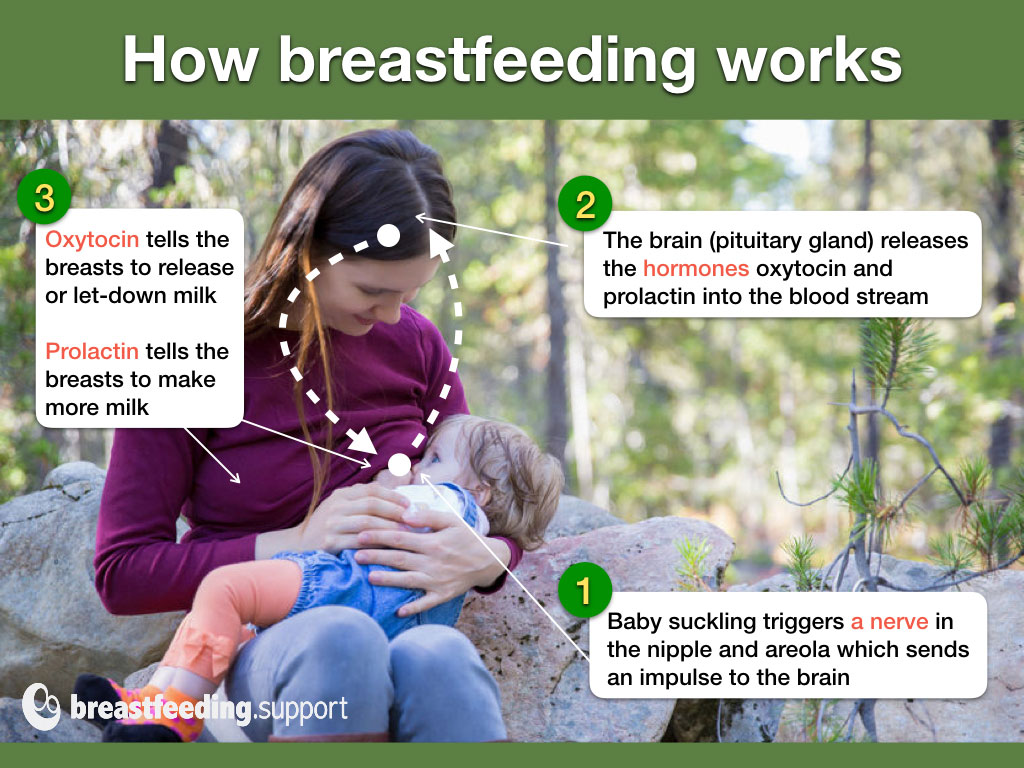
How breastfeeding works. A infant sucking stimulates a nerve past the nipple to transport a message to the brain to release specific hormones (oxytocin and prolactin). Oxytocin signals chest milk to be released (let-downward) from the milk-making tissue in the breast and then that the milk is carried to the nipple through little tubes (ducts). Prolactin signals milk product. Any damage to the nerves, ducts or glandular tissue tin can affect how breastfeeding works subsequently chest reduction surgery.
#1 Type of surgery
During breast reduction surgery part of the breast will be physically removed and this could affect milk supply in a number of means:
- Cutting across important nerves tin can reduce nipple sensitivity and affect the neurohormonal reflex that triggers milk production and let-downward.
- Cutting through milk ducts means that areas of the chest may become engorged and ultimately close down milk production because at that place is no outlet for the milk.
- If the nipple is removed and and so placed on a reconstructed breast, the resulting damage to the nerves, milk ducts, and breast tissue will impact breastfeeding significantly.
- Scarring within the breast may affect lactation. The scar blueprint on the surface of the chest does not reveal the type of surgery.
Surgical techniques
Several surgical techniques are possible for breast reduction and some volition accept more than impact on breastfeeding than others. The best chance for breastfeeding success will be where the procedure leaves the nipple and areola attached to the chest tissue beneath them. Lactation consultant Diana West has outlined a selection of techniques in her bookDefining Your Ain Success Breastfeeding After Breast Reduction Surgeryand these are summarised below:
- Fat removal (liposuction).Cuts are made in the breast to insert a suction tube to remove fatty deposits from areas of the breast. This may harm glandular tissue depending where the tube is inserted, and may crusade scarring simply is idea to be the least dissentious technique for breastfeeding.
- Anchor blazon or inverted-T (inferior pedicle technique) involves removing sections of the breast and repositioning the nipple. The nipple is left on a mound of tissue (pedicle) so that it still has its nerves, blood supply and ducts intact. More glandular tissue may be retained with this technique compared to others which helps to preserve some caste of breastfeeding later. The surgery leaves a scar running around the areola (the darker skin around the nipple), a vertical scar from nipple to the chest wall, and so a horizontal scar under the breast in the crease where the breast meets the breast wall (inframammary crease or fold) making an anchor shaped scar.
- Effectually the areola (periareolar) technique involves making an incision around the areola and pulling out breast tissue through the incision. Glandular tissue will be removed along with fatty tissue and important fretfulness may be damaged.
- Fundamental mound technique preserves the nipple and areola. Nonetheless there is probable to be considerable impairment to the glandular tissue due to the specific methods involved in reshaping the breast.
- Periareolar with mesh back up (or "double skin") involves a similar technique to the periareolar technique above notwithstanding a constructed mesh is inserted in the breast to provide support and reduce postal service surgery sagging. The technique can remove large amounts of glandular tissue and important fretfulness may be damaged.
- Superior pedicle technique (or "Lejour") preserves the nipple-areola complex merely can impact on the nerves and ducts as it removes a meaning amount of glandular tissue directly beneath the nipple.
- Free nipple graft involves complete removal of the nipple and grafting it back to a new location on the remodelled breast. All nerves and ducts will be severed causing pregnant damage to breastfeeding and affecting nipple awareness. Even though establishing a milk supply is unlikely, information technology is possible for some fretfulness and ducts to reconnect and some sensitivity to returnone.
#2 How much glandular tissue remains?
Glandular tissue in the chest is interspersed with fatty tissue and it is not possible to say past just looking at the size of a chest how much glandular tissue is present before or after surgery. Therefore we tin can't presume a large breast has more glandular tissue than a small breast or that a big breast can afford to exist halved by surgery and still be functional. How breast reduction can affect milk-making capacity depends on how much functional glandular tissue is left after surgery. The more than glandular (milk-making) tissue that is removed by surgery, the more likely information technology is that breastfeeding (milk supply) will exist affected.
#3 How much time has passed?
Equally time passes after chest reduction surgery, damaged nerves may reconnect (reinnervation) and severed ducts may make new connections to the nipple (recanalisation). Nipples that had lost any sensitivity may become more sensitive again and the capacity of the breast to make milk may amend.
Healing of milk ducts (recanalization)
Some milk ducts that have been cut or damaged seem to reconnect or develop new pathways to carry the milk to the nipple. The hormones of pregnancy and to an extent the catamenia cycle tin also help with development of new glandular tissue. Breastfeeding also helps this process—with each new breastfeeding experience there can be a niggling more recovery and a meliorate milk supply. Recovery will be limited by how much breast tissue remains and how many milk ducts.
Researchers institute an average of nine ducts that came all the way through the nipple, but every bit few as four were as well observed. A woman with nine ducts can afford to lose a couple, but a woman with only four really tin't beget to lose any. Though she may all the same have enough milk-making power, if the milk can't get out and then baby can't go it and that area of the breast will stop producing.
Healing of nerves (reinnervation)
An important nerve for triggering the release of prolactin and oxytocin is the quaternary intercostal nerve. If this is damaged it affects let-downwards and milk product. Co-ordinate to bfar.org, a website defended to breastfeeding later on breast reduction, damaged fretfulness can repair and reconnect at a growth rate of 1mm per month irrespective of breastfeedingtwo. A expert sign that this is happening volition be when any lost sensitivity to touch and temperature returns to the nipple.
It generally takes about five years for nerves to grow dorsum to meaning or full functionality.
Ofttimes asked questions
Will I have enough milk?
Although some women manage to breastfeed successfully, there is a strong possibility that yous won't take a full milk supply, especially for the start baby born afterward chest reduction surgery. It will be important to keep a close eye on your baby's weight gain and nappy output to estimate their milk intake. It may be necessary to supplement your babe. An IBCLC lactation consultant can help you optimise your milk supply and see A Good Start to Breastfeeding and Is My Baby Getting Plenty Milk?
What if supplements are needed?
It'south important that your baby is well fed to requite them enough energy to breastfeed and preclude jaundice or dehydration, and then supplements of donor milk or formula may be needed. Although you lot may non be able to make a full supply of milk, any amount of breast milk you tin provide volition be beneficial to your baby. Breastfeeding is a relationship, not just a way to feed a babe, and so comforting your baby at the chest and holding your baby in pare-to-pare contact will be valuable even if you don't have much milk.
If yous demand to supplement, options include:
- A supplemental nursing system. This allows a mother to supplement her baby directly at the breast using a feeding tube, meet photo beneath and Breastfeeding With a Supplemental Nursing System
- Finger feeding. Tiptop ups to supplement breastfeeding could be offered short term by finger feeding encounter What is Finger Feeding?
- Canteen. At that place are lots of ways to make a canteen feed more like a breastfeed so that a baby doesn't go confused past switching betwixt breast and canteen see our Tips to Canteen Feed a Breastfed Baby and Best Canteen for a Breastfed Baby.

How can I maximise my milk supply?
See A Good Start to Breastfeeding and Breastfeeding Tips for Newborns for general ideas to get breastfeeding working well and see our tips below:
Before the nativity
Discuss antenatal expression of colostrum with your health professionals and see Expressing Colostrum Antenatally.
The get-go 60 minutes
Spending time in skin-to-peel contact and breastfeeding in the offset hr after nascency has many advantages for mother and baby including helping a milk supply. If baby isn't ready to latch on, hand expressing tin can remove milk instead of baby. This video by Jane Morton explains why the first 60 minutes is important for milk supply: A Mother'southward Bear on Breastfeeding in the Showtime 60 minutes.
Frequent feeds
Frequent breastfeeding or hand expressing (at least every two hours, more than if yous can) will aid stimulate your milk supply. It may be useful to pump afterward breastfeeds for a few weeks in one case your milk is in to maximise your supply.
Comfortable breastfeeds
Ensure breastfeeding doesn't hurt, come across Latching Tips and Breastfeeding Positions for Newborns.
Making more milk
There are lots of ways to increase a milk supply including frequent pumping with a hospital grade pump, using both breasts per feed, breast compressions, and frequent feeds. It tin can be very useful to see an IBCLC lactation consultant to help you lot as in that location can be other Reasons for Low Milk Supply, not just the surgery. Run into How to Brand More Chest Milk and How to Increase Milk Supply by Pumping.
Galactagogues
A galactagogue is a food, herb or drug that might assist to increment milk supply or assistance promote more glandular breast tissue. For much more than information run across What Is a Galactagogue?

What difficulties might I expect after surgery?
Certain difficulties may present themselves if you have had chest surgery. But bear in mind these problems tin come along at whatsoever time and may non be to practice with the surgery at all—cheque with an IBCLC lactation consultant or breastfeeding specialist.
Severe engorgement when milk comes in
Some breast engorgement (feelings of fullness and swelling) after birth is normal. Engorgement is non just from milk but includes tissue fluid and blood in the breasts. Engorgement is a adept sign that functional milk-making tissue is still nowadays. Still some milk ducts may be blocked due to the surgery or scarring. 1 breast may be more engorged than the other. Areas of the breast that are non able to drain will shut downwards milk production. Engorgement may be worse with second and subsequent babies specially after a long and successful breastfeeding experience previously. Try to remove as much breast milk as possible to salvage the engorgement and run into Engorged Breasts, and Engorgement Relief When Milk Won't Flow.
No engorgement when milk comes in?
There tin be several reasons for milk not coming in after delivery in addition to removal of glandular tissue by breast surgery. Meet No Breast Milk After Delivery and contact an IBCLC lactation consultant for assist and back up.
Reduced nipple sensation
If you do not take any sensitivity in your nipples information technology can exist harder to initiate the let down, but there are ways to status this response to other triggers, see Let-Downwards Reflex: As well Slow? past Kelly Bonyata.
Nipples painful, sore, or white
Mothers who have had nipple or breast surgery are more than at run a risk of nipple vasospasm (sudden narrowing or constriction of blood vessels in the nipple accompanied past pain). This is perhaps due to trauma to the claret supply and nerves (bfar.org, 2022). As nipple vasospasm tin have other causes such as poor attachment, positioning, certain drugs—including caffeine and nicotine—or Raynaud'due south Phenomenon, it is of import to rule out all causes. See Nipple Vasospasm and Breastfeeding for more data on treatments and prevention and check wth your breastfeeding helper.
Hurting in the breasts
Adhesions in the breast (scars) may exist a cause of pain and may inhibit the let-down. There are other causes of pain to dominion out all the same. Thrush or bacterial infections, mammary constriction syndrome and poor latch can all create deep breast pain.
When an adhesion is suspected, the first remedy is to try to move the layers of tissue by frequent, gentle massage, which will break the adhesions if they are non too dense. In the case of nipple adhesions, the nipples tin can be gently pulled outward. With fourth dimension and agile employ of the chest, the adhesions will usually diminish in severity.
Considering chest reduction surgery?
Breast reduction surgery can cause difficulties breastfeeding and many women will not be able to brand a total supply of breast milk. If you accept not already had breast surgery you will want to consider this fact alongside the other medical risksthree. Breastfeeding may not seem important to y'all now, but this might change when you approach motherhood. Although there are ways to minimise the touch on on breastfeeding when performing surgery this is non a guarantee to success and non all breast surgeons consider protecting breastfeeding without prompting.
What should the surgeon say to the woman request for chest reduction surgery? That the chances that she will exist able to breastfeed her babies exclusively are depression. And if this woman is 16 or 17 years old, maybe it'southward better to wait a few years, considering the surgery cannot be undone, and perhaps in a couple of years she may have a different outlook on life.
The surgeon should conspicuously discuss the options with the patient or provide a procedure that leaves the ducts intact. If the ducts are intact, breastfeeding can be successful postoperatively. The nerve must also be intact for tactile sensations to trigger let-down.
Support groups
Good support tin can be essential for maximising your milk-making potential. Contact an IBCLC lactation consultant for one-to-1 help and for online customs support visit Breastfeeding Later on Reduction (BFAR) and BFAR UK Support Grouping (Facebook groups).
Summary
Breast reduction surgery can present several challenges for breastfeeding. Even so a mother may be able to make a full or partial milk supply depending on the type of surgery, amount of functional breast tissue removed and the fourth dimension that has passed since surgery. It is important to make certain breastfeeding gets off to a good start to maximise a milk supply subsequently a surgical procedure. An IBCLC lactation consultant or breastfeeding specialist is an platonic support person to help with this so that whatsoever breastfeeding problems unrelated to your surgery tin can be ruled out and your breastfeeding potential can be maximised.

Can Damaged Milk Ducts Repair Themselves,
Source: https://breastfeeding.support/breast-reduction-and-breastfeeding/
Posted by: swearingendishice.blogspot.com
0 Response to "Can Damaged Milk Ducts Repair Themselves"
Post a Comment